With much frustration, patients often bounce from one medical doctor to another to find the source of their discomfort. Negative or inconclusive findings often lead to prolonged drug therapies, and often an ultimate and incorrect diagnosis of psychosomatic illness. Our dentists have the experience to diagnose and treat complex conditions of the TMJ and other areas of the head, face, and neck. Call 212-452-3344 or visit our website to arrange an evaluation with NYC Smile Design today.
What Is Neuromuscular Dysfunction?
Your “incurable” headache, ear and facial pain could be coming from jaw joints, your bite-how your teeth meet and/or spasms in your facial musculature. Our practice approaches treatment and management of problems of this nature as a team with your physician to provide the most comprehensive solutions. We are committed to the long term benefits of comprehensive neuromuscular treatment and enthusiastic about the options offered by the advanced technology that is part of the process.
TMJ vs. TMD
TMJ stands for our left and right temporomandibular (jaw) joints. The acronym TMJ is very often incorrectly used to describe a disorder of these joints. However, the correct acronym of the disorder is TMD, meaning temperomandibular disorders and when we include the many symptoms of head, neck, facial and jaw pain it is recognized as “craniomandibular disorders.”
Long term studies now prove that the following symptoms are linked to the incorrect alignment of the upper (maxilla) and lower (mandibular) jaws and changes in the integrity of the TMJ. This produces physiologic stress, pain and dysfunction in the joints, supporting ligaments and associated muscles:
- Headaches
- Dizziness facial, neck, or back, pain
- Pain or soreness of the jaw joints clicking, popping, or grating sounds as jaw joints are in motion
- Congestion or stuffiness of the ears
- Numbness of the arms and fingers, chipped, or cracked teeth
- Pain in teeth that seems to move around
- Loose teeth
- Ear pain
- Ear ringing/ buzzing sounds in ear
- Loss of auditory acuity
- Limitations of motion of jaw joins
- Jaw locking upon opening or closing
- Tired face/jaw
- Snoring
- Difficulty swallowing
- Tingling fingers/hand numbness
Left untreated, the problems progress, getting worse over time and the stress and tension it produces can cause everything from mild discomfort to severe chronc pain throughout the body.
Craniomandibular disorders can also exacerbate:
- Fibromyalgia
- Tinnitis
- Migraine
Causes of Neuromuscular Dysfunction
The Exact Cause of TMJ is Not Always Known. The factors responsible for craniomandibular disorders may be single or multifactorial. These include:
- Developmental: A malrelationship of the maxilla and mandible produces symptoms that may emerge during childhood or may not occur until adulthood after years of day to day trauma.
- Improper occlusion/bite: When teeth do not fit together properly it causes sustained microtrauma to the joints. Over time the body compensates by involving other muscles of the body
- Direct trauma to jaw
- Indirect trauma to jaw: A significant number of cervical whiplash injuries are accompanied with mandibular whiplash-a stretching or tearing of the ligaments of the jaw joints and cause damage within the supporting musculature.
- Tooth loss: Losing teeth without adequate replacement results in a change in jaw position; improper restorations that change the jaw relationship or make an incorrect one worsen.
- Poor sleep habits/position
- Poor posture: Places unnecessary wear and tear on all joints, including jaw joints and resulting damage is similar to direct trauma
- Bruxism/clenching of teeth: Some patients do this unconsciously and in some patients we are uncertain why this is occurring. This produces stress on jaw joints and muscles of face and neck
- Sleep apnea: It is theorized that some patients clench and brux their teeth unconsciously to maintain the muscles of the throat and mouth in a patent open airway. This will help maintain an airway but will put stress on jaw joints and muscles of face.neck
- Stress: Some patients unconsciously brux and or clench their teeth in response to increased stress
Classification
Craniomandibular disorders are classified as intracapsular or extracapsular. Intracapusular Disorders are characterized by structural alterations in the joint itself.
Intracapsular:
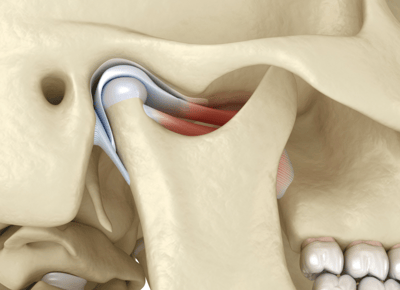
You Don’t Have to Live With Pain. The normal physiologic relationship between the part of the lower jaw called the condyle, the disc that moves between it and the part of the skull called the fossa have been altered and compromised. This interferes with form and function and frequently produces pain.
Degenerative osteoarthritis, rheumatoid arthritis and neoplasms are intracapsular disease. Trauma induced to the joint directly or indirectly can result in intracapsular disorder. A common problem is a slipped or dislocated disc of the jaw joint. Due to tearing or stretching of the disc and its attachments the disc assumes an abnormal position forward of the condyle instead of cushioning the condyle with the fossa.
Opening movements produce a clicking sound as the disc slips back into the proper position (a process called disc reduction) momentarily over the condyle. Frequently upon closing, as the disc assumes its abnormal position and slips off the condyle forward of it click can be heard again. These clicks may be audible, but frequently require a stethoscope or sophisticated instrumentation to hear it.
If this anterior disc displacement is left untreated, it may ultimately result in an “anterior disc displacement without reduction” meaning the disc never goes between the condyle and fossa. This causes limitations in movement laterally and opening and is called “closed lock” as the disc now acts a mechanical obstruction, getting in the way for normal condyle movement.
Long term worsening frequently results in degenerative osteoarthritis producing severe alterations in form and function. Most often internal/intracapsular problems/ derangements produce pain from the joint itself with or without referred pain to other areas of the head or muscle dysfunction such as spasm and myofascial trigger points.
Extracapsular:
Extracapsular disorders occur when the musculature of the TMJs have an altered acquired postural rest position. Over a prolonged period of time the muscles maintain themselves in an altered state of hyperfunction which the brain perceives as an accommodated “balanced position.”
This change from a physiologic rest position to an accommodated rest position occurs when the mandibular trajectory of closure is not coincident with the TMJ/neuromuscular trajectory of closure. This trajectory is directly affected by how the teeth meet-their “occlusal relationship” and how their proprioceptive input causes a change in jaw position forcing muscles to function at less than their optimal lengths.
This all results in the musculature and TMJs existing in a “stressed” condition. The subjective symtoms are similar to intacapsular problems including joint pain as well as muscle dysfunction such as spasm and myofascial trigger points. No joint noises are found with extracapsular disorders.
A strong and direct biomechanical relationship exists between all the muscles of the head and neck. As a result of reciprocal muscle function, dysfunction and pain in the head and face muscles, frequently results in dysfunction and pain in the cervical muscles-neck pain- that can eventually involve the whole upper back. Due to unbalanced posturing of muscles of the head neck and shoulders, these patients maintain what is called a forward head posture.
Neurologically there is a strong relationship between the head and neck muscles and the ear. Ear symptoms, including congestion, pain, buzzing, ringing and even loss of hearing are frequently found in craniomandibular disorders.
The best way to treat these symptoms is to establish their origin, by using the sophisticated diagnostic techniques of neuromuscular dentistry, evaluating the results to determine the best course of treatment. These can include orthotics, orthodontics, correction of existing restorations — all the way up to full-mouth rehabilitation where indicated for orthopedic and musculoskeletal stabilization. Finding the best treatment for them not only repairs the damage that has been done, but also prevents them from getting worse and stabilizes their physical condition at its optimal point.Neuromuscular Treatment
You are central to the process: The more accurately you describe your symptoms (and your goals), the more precisely we can test for and diagnose the best course for treating and attaining them. When a patient chooses the benefits of the diagnostic process, they can look forward to a thorough discussion of the test results in order to be able to select the options that seem most promising for long-range comfort. The process works like this:
- At our initial consultation, we make detailed notes of all the chronic symptoms you experience.
- Next, using the most sensitive cutting-edge technology, we record and interpret the sounds of both your left and right TMJs in motion with computerized electrosonography to objectively determine the pathologic nature and extent of joint sounds. In addition, we measure the pre and post relaxation status of muscles with highly sensitive electromyography (EMG) that records the electrical activity of your facial and neck muscles.
- A computerized jaw scanner is used to track the spatial movement of your jaw as you open and close. TMJ X-rays show us any pathology that may or may not exist, changes to bone structure and the position the lower jaw is in with your skull. These measurements enable us to map out all your unique facial, bone, and muscle tissue functions.
- By determining where you are presently, we can then move on to the next step- finding the most relaxed position of your jaw.
Finding that most relaxed position from which your muscles will act most efficiently and comfortably is accomplished through the use of a TENS machine. Once it has been confirmed, our goal for the first stage of the treatment will be the maintenance of this position. This position can be maintained through the use of occlusal guards and orthotics.
The second stage of the treatment begins once your symptoms are diminished, and we are assured that our goal of establishing the most comfortable position has been accomplished. The goal of this stage is also to create a bite that will preserve the corrected alignment of the jaw so that jaw, muscles, and teeth can work together in harmony. Completion of the second stage will include decisions about future use of any guards, orthotics and/or orthodontics as well as the benefits of full-mouth rehabilitation.
After choosing the direction of the treatment, we begin by creating a jaw position for the remainder of treatment. This can be accomplished in several ways: with a removable orthotic or a fixed orthotic, or can be achieved by moving the teeth through orthodontic treatment. Once the position has been stabilized we move to the second stage of treatment previously agreed upon.
Don’t live with pain a day longer than you have to. Find out how our experienced neuromuscular dentists can help by calling 212-452-3344 or visit our website.